
Table of Contents
Background:
- Approximately 80% of maternal deaths globally are due to obstetric complications.
- 99% of all maternal deaths occur in developing countries.
- Maternal mortality ratio in developing countries in 2015 was 239 per 1,00,000 live births.
- Millions of births are not assisted by a midwife, a doctor or a trained nurse.
- Every day, approximately 830 women die from preventable causes related to pregnancy and childbirth.
- Many of these complications are preventable, avoidable and resolvable.
History:
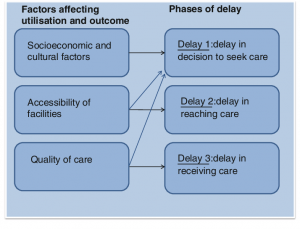
In 1994, Sereen Thaddeus of the United States Agency for International Development (USAID) and Deborah Maine, Professor Emerita at the Columbia University Mailman School of Public Health, linked causes of maternal mortality to “three delays”; delay in seeking care, delay in arrival at the health facility, and delay in the provision of adequate care.
The field of maternal mortality reduction has long used the framework of the 3 delays to understand barriers to care and to identify points of intervention.
Three delays:
1. Delay in the decision to seek care (Seeking care);
2. Delay arrival at a health facility (Reaching care); and
3. Delay in obtaining the adequate treatment (Receiving care)
1. Delay in decision to seek care (Seeking care):
- Delay #1 is recognizing a problem and deciding to seek medical attention.
- If the community or a household is aware of a functioning referral system, and what it might cost them, if anything, the decision to seek care might happen faster.
- It is the delay in seeking health care by the husband, family members or the patient herself.
- It usually occurs when one fails to recognize the danger signs and symptoms
This delay mainly occurs due to:
- Lack of the knowledge on the outcomes
- Financial constraints.
- Women not in a position to make decisions
- Lack of encouragement among family members to the health facility
- Fear from ill treatment, or the medical procedure
- Fear of getting recognized for some severe disease on going to health facility
- More trust on home remedies than seeking health care services
- More priority on household works or other works than own health.
- Poor standards of care in health facilities
- High out of pocket expenditure in health facilities
2. Delay in the arrival of health facility (Reaching care)
- Delay #2 occurs reaching a facility. This delay is predominantly determined by physical and financial accessibility to health services: their geographical distribution and location, distance and road conditions, the availability of transportation and its cost.
- It is the delay in reaching to the health facility once the decision to seek care is taken.
- Delay in decision to seek health services already adds up to this delay.
This delay mainly occurs due to:
- Very distantly/remotely located heath facilities
- Lack of means of transportation
- Lack of emergency means of transport (ambulance)
- Emergency transport delays and refusals
- Wait for someone else to accompany women in the journey
- Financial problem making ambulance unaffordable and relying on public transportation.
3. Delay in obtaining the treatment in the facility (Receiving care)
- Delay #3 happens once she has arrived at a health care facility, if staff aren’t available, or equipment is broken, or blood needs to be donated.
- It refers to the delay in initiating appropriate treatment once the patient reaches to the health facility.
This delay mainly occurs due to:
- Lack of emergency preparedness in facilities.
- Lack of equipment, supplies, drugs.
- Lack of adequately trained staff/s.
- Poor attitudes of staff (discrimination based on color, creed, wealth, etc.).
- Complex legal formalities to be followed before starting treatment.
- Weak referral system without proper documents.
- Lack of accountability during referrals.
Consequences of Three delays:
- Delay in seeking care further increases the complications of the patient and creates life-threatening situation.
- Delay in reaching the health facility will leave health workers with limited scope to take actions
- Delay in receiving health care would demotivate the care seeker. Moreover, it can later affect the health seeking behavior of a person.
- ‘Three delays’ is directly linked with the maternal morbidity and mortality.
Possible Interventions to Prevent or Mitigate Three delays:
With a strong communication system in place as a key piece of the overall referral system, it is possible to call the receiving facility to alert them that someone is being referred and triage is ready and waiting. More specifically, each delay can be addressed in following ways:
i) Delay in decision to seek care:
- Raise knowledge and awareness of danger signs and where and when to seek care during pregnancy, postpartum and neonatal care.
- Facilitate income generation and referral through local health workers
- Improved communication with the community people and local leaders.
- Provision for financial incentives for seeking care.
- Counselling the pregnant women and mother-in-law for seeking health care regularly and periodically during pregnancy and postpartum period.
- Empower women and increase decision-making power of mother.
ii) Delay in the arrival of health facility
- Mobilize/provide transportation facilities to the pregnant women.
- Make health services accessible in every part.
- Bring appropriate care closer to community.
- Proper mobilization of the community health workers.
- Funds to cover or minimize costs.
- Conduct outreach camps.
- Provision of mobile ambulances.
- Provision of stand-by local vehicles for taking the women to health facility whenever required in consultation with the local people and leaders
iii) Delay in obtaining treatment in the facility
- Provision of adequate equipment and supplies.
- Improve staff availability.
- Ensure the availability of drugs.
- Improving staff capacity through trainings and workshops.
- Regular monitoring and supportive supervision from the higher authorities.
- Strengthen the referral system.
References and for More Information:
https://borgenproject.org/the-three-delays-maternal-mortality/
https://www.ncbi.nlm.nih.gov/pubmed/8042057/
http://www.who.int/news-room/fact-sheets/detail/maternal-mortality
https://www.sciencedirect.com/science/article/pii/S2214109X1470227X
https://www.jica.go.jp/project/philippines/0600894/04/pdf/ppt_03.pdf
Upadhyay R, Rai S, Krishnan A. Using Three Delays Model to Understand the Social Factors Responsible for Neonatal Deaths in Rural Haryana, India. JOURNAL OF TROPICAL PEDIATRICS. 2013;59(2).
http://www.acrwebsite.org/search/view-conference-proceedings.aspx?Id=7203
https://www.healthynewbornnetwork.org/hnn-content/uploads/Applying-the-three-delays-model_Final.pdf
https://academic.oup.com/heapol/article/31/9/1152/2452980
https://www.maternityworldwide.org/what-we-do/three-delays-model/
https://www.unfpa.org/sites/default/files/pub-pdf/reducing_mm.pdf
https://www.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=16404&lid=3
https://www.tandfonline.com/doi/full/10.1016/S0968-8080%2812%2939601-8