
- Prevention of Mother to Child Transmission (PMTCT) is a commonly used terminology for preventing the transmission of HIV virus from pregnant mothers to their infants
- It refers to the set of programs/interventions designed to identify the pregnant mothers with HIV and provide them with effective interventions to prevent mother to child transmission (MTCT)
- PMTCT is an intervention to ensure that no child is born with HIV. Thus, this approach is envisioning and approaching towards an AIDS free generation
- MTCT is a burning issue in HIV and AIDS as 90% of new cases of HIV in infants and children’s are due to MTCT
- PMTCT approach mainly uses Anti-Retroviral Therapy (ART) along with other preventive methods and interventions in cases of breast feeding, child delivery etc. to prevent the transmission of virus to the infants
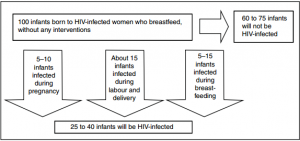
- Mother to child transmission of HIV virus may occur at three different points. They are:
- During Pregnancy
- During Labour and delivery
- During breastfeeding
- Although mother to child transmission of HIV virus is always dangerous and risky, it is necessary to know that HIV virus doesnot transmit from infected mother to child in all 100% cases. Even if no ART or other PMTCT approaches are taken, chances of MTCT is around (25-40)%.
- The figure below explains about the chances of MTCT of HIV virus at different times:
- As the probability of Mother to Child Transmission of HIV virus (from HIV infected mothers) is as high as 25% to 40%, PMTCT approach decreases this risk by a substantial amount
- To be precise, if HIV infected mother and child both have received ART and the children is only breastfed for first six months of life:
- 95% or more children will be not be infected with HIV
- 2% children might still be infected during pregnancy, labour or after birth and
- 3% children might get infected during breastfeeding
- Apart from different mode/points of transmission of virus, there are certain risk factors which increase the risk of transmission and may put women at a higher risk of transmitting the virus to her children.
- The risk factors are:
- The viral load in the mother’s blood i.e. amount of HIV virus in the blood. The more the viral load, higher are the chances of transmitting virus to the infant
- Maternal, obstetrical, viral, fetal and infant related factors
- The current WHO guidelines recommend two interventions:
- Providing lifelong ART to all pregnant and breastfeeding women living with HIV regardless of CD4 count or clinical stage or
- Providing ART (ARV drugs) for pregnant and breastfeeding women with HIV during the mother-to-child transmission risk period and then continuing lifelong ART for those women eligible for treatment for their own health.
- Some of the core interventions for PMTCT and the way it works for reducing MTCT can also be understood from the table below:
| PMTCT core interventions | The way intervention works |
| HIV testing and counseling | Identify women infected with HIV |
| Antiretroviral treatment and prophylaxis | Reduces maternal viral load |
| Safer delivery practices. May also opt for elective caesarean section, if safe and feasible | Reduces infant exposure to virus during labour and delivery |
| Safer infant-feeding practices | Reduces infant exposure to virus through safer feeding options |
- Considering all the risks and complexities of MTCT, PMTCT interventions are designed in a more comprehensive and holistic way.
Comprehensive PMTCT:
- Comprehensive PMTCT approach/program provides continuum of care for both mother and child. The continuum of care includes:
- Educating adolescent women about primary prevention of HIV infection followed by
- Treatment, care, and support to women who are HIV positive and their families.
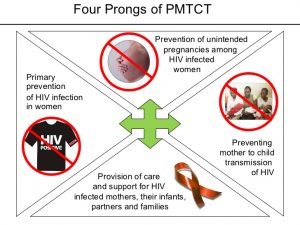
- There are basically four elements of comprehensive PMTCT programs which are also promoted by World Health Organization. They are:
Guidelines for HIV exposed infants:
- Infants born to mothers living with HIV should be immediately given a dose of Anti Retroviral Therapy just after birth. The treatment of the child should be in line with mother’s course of ART drugs and infant feeding method.
- At 4-6 months, the infant (born to HIV infected mother) should be given early infant diagnosis
- Lastly, another/final infant diagnosis should be done at 18 months/after stopping breast feeding
Ensuring effective PMTCT:
Effective PMTCT requires mother and babies to:
- Have ANC checkup and HIV testing during pregnancy
- Have access to antiretroviral treatment (ART)
- Practice safe childbirth practices and appropriate infant feeding
- Make use of infant HIV testing and other post-natal healthcare services
References:
https://www.cdc.gov/globalaids/resources/pmtct-care/docs/pm/module_2pm.pdf
https://www.avert.org/professionals/hiv-programming/prevention/prevention-mother-child
http://apps.who.int/iris/bitstream/10665/208825/1/9789241549684_eng.pdf?ua=1
https://aidsfree.usaid.gov/resources/pkb/biomedical/prevention-mother-child-transmission-hiv-pmtct
http://www.who.int/hiv/pub/mtct/PMTCTfactsheet/en/
http://www.who.int/gho/hiv/epidemic_response/PMTCT_text/en/
https://www.unicef.org/supply/index_42855.html
https://red.org/what-is-pmtct/
http://www.psi.org/program/prevention-of-mother-to-child-transmission-intervention/
http://www.pedaids.org/pages/pmtct-impact
https://www.k4health.org/toolkits/pmtct/pmtct-strategies
http://sustainuganda.org/content/prevention-mother-child-transmission-pmtct
https://www.westerncape.gov.za/service/prevention-mother-child-transmission-pmtct
http://www.emtct-iatt.org/wp-content/uploads/2013/04/Nigeria_National-PMTCT-Guidelines_2010.pdf
http://www.wvi.org/health/pmtct-approach
http://www.nas.gov.sl/interventions/pmtct
http://www.givewell.org/international/technical/programs/PMTCT
https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-11-426
http://www.unaids.org/en/resources/presscentre/featurestories/2016/october/20161024_EMotherToChildT
http://www.lifestitches.org/project/pmtct.html
http://www.unaids.org/en/resources/presscentre/featurestories/2010/april/20100421whostrategypmtct
https://www.one.org/us/2010/09/16/how-do-you-prevent-mother-to-child-transmission-of-hiv/